
Cruciate Ligament Disease
What is the cranial cruciate ligament?
There are four main ligaments in the stifle (knee joint) of a dog; two outside called the collateral ligaments and two inside the joint called the cruciate ligaments. The cruciate ligament nearest the front of the joint is the cranial cruciate ligament (CCL), the equivalent to the anterior cruciate ligament or ACL in a human. The ligament attaches the femur (thigh bone) and to the tibia (shin bone), preventing the tibia from moving forward relative to the femur. It also helps to prevent over-extension and rotation. The caudal cruciate ligament is responsive for the opposing movement, principally stopping backwards movement of the tibial relative to the femur.
Why do dogs get cruciate ligament problems?
Most commonly, the ligament is injured in dogs due to a degenerative breakdown. This is in direct contrast to people where trauma is usually at fault.

Arthroscopic view of an unhealthy, partially torn cranial cruciate ligament
Although this is a common ailment, we do not fully understand why this condition develops in dogs. We know some breeds are more commonly affected (Labradors, Rottweilers, Golden Retrievers, Boxers) and some breeds are relatively protected (greyhounds & whippets). The exact cause remains unclear. Some breeds may have conformational abnormalities which predispose to this condition (Bichon Frise or West Highland White terriers). They have similar tibial anatomy which increases pressure on the ligament. As this is a degenerative condition, we often use the term ‘cranial cruciate ligament disease’ rather than ‘cranial cruciate ligament rupture’.
What are the signs of cruciate ligament disease?
The most common sign of cranial cruciate ligament disease is hind limb lameness (limping). In dogs this can occur suddenly but in others it may develop slowly. There is a lot of variation in the degree of lameness; some dogs cannot put any weight on the leg, whereas others only have a subtle limp. In cases where both left and right ligaments are affected simultaneously, dogs won’t limp. Rather, they are prone to sitting down routinely, have trouble jumping and they often look like they are lifting themselves from the ground using their front legs only. Some dogs show stiffness after rest and others get worse after exercise.
How is cruciate ligament disease diagnosed?
A diagnosis can be straightforward if the ligament is completely ruptured and is usually confirmed on examination by an experienced orthopaedic surgeon. The most useful test is palpation of the stifle to confirm instability which identifies abnormal movement typical of ligament failure. When a partial tear is present this can be more difficult to diagnose as there is not the same degree of instability in the joint. In these cases, other tests may be required such as radiography (x-rays) and assessment under anaesthesia / sedation. Radiographs may show signs consistent with the presence of osteoarthritis which is commonly present in dogs with cranial cruciate ligament disease. In most dogs, exploratory surgery or arthroscopy (keyhole surgery) is used to confirm the ligament is damaged. The cartilage in the joint will also be assessed as meniscal (cartilage) damage can often occur along with CCL disease.

Arthroscopic view of a meniscus
Conservative management options
This type of management uses weight control, exercise control, rehabilitation, non-steroidal anti-inflammatory drugs and dietary supplements. However, this offers a very unpredictable outcome and for this reason it is not commonly recommended in our clinic. Dogs undergoing this management may improve in the earlier phases of treatment, but longer term outcomes are often poor. Small dogs may respond better than bigger dogs, but again the outcome is unpredictable.
Surgical management
Many different techniques have been described for treatment of this condition and the outcomes were considered similar for a long time. However, there is a growing body of evidence which supports plateau levelling procedures in all size dogs.
Tibial Plateau Levelling Osteotomy (TPLO)
The TPLO procedure does not rely on the presence of the ligament, but instead changes the forces in the joint to create a more stable ‘platform’ when the dog is weight bearing on the leg. A semi-circular cut is made in the top of the tibia (shin bone) and the top section of bone is ‘levelled’ to improve stability in the joint. The cut bone is stabilised with a bone plate and screws. Once the bone is healed, the procedure is complete. Although the bone is cut, this is a well tolerated procedure with many dogs weight bearing on the leg within 48 hours of surgery.
At Queensland Veterinary Specialists, we are experts in this procedure, with our specialists involved in training other veterinarians in this technique. We use the highest proven quality in locking implants, using principally Synthes equipment which is an industry leader in human and veterinary orthopaedics. We can offer this technique in all size dogs, from Papillions to Great Danes with success rates exceeding 95%.

Cranial closing wedge ostectomy (CWO)
This technique also levels the top section of the tibia in a similar way to TPLO, but by removing a wedge of bone rather than using a curved cut. This was the predecessor surgery to TPLO and is occasionally used in some patients. The bone is again stabilised with a bone plate and screws.
Tibial Tuberosity Advancement (TTA)
This technique also uses a cut in the top of the tibia (shin bone), but in this case the front of the knee is ‘pushed’ forwards to change the forces in the knee.
TTA procedures are also known by the following names:
MMP
TTA-2
JUMP
TTA Rapid
All of these procedures share the same premise of action. They are designed to alter the pull of the quadriceps but are disappointingly associated with higher rates of post operative instability, meniscal injury and ongoing lameness.

Which technique is best?
There is alot of mis-information out there on whether one technique is superior or not, and whether one is ‘safer’ or more ‘risky’ than another. We are very proud at QVS, that as trained specialists we are able to have an open and honest conversation about our case experiences and have a strong understanding of the breadth and depth of scientific literature that guides decision making for individual cases with cruciate disease.
We are also happy to show you the published evidence that supports our decision to offer TPLO surgery in the great majority of cases. Our surgeons have extensive training in cruciate surgery and are trained in offering all modern techniques (TPLO, TTA, CBLO, Lateral suture, TTO). The reason we recommend TPLO, over other techniques is its documented published success relating to:
low late meniscal injury rates
low infection rates
extremely rare implant related issues
no history of significant post operative fractures
Additionally, this seminal publication comparing outcomes supports TPLO as providing post operative leg use that is similar to dogs without any cruciate disease by 6 and 12 months post operatively. If you follow the graph, the Hind limb symmetry index (VI) is a measure of whether the left and right leg use is equal. The goal is that the operated limb reaches 1. You can see on the below graph that TPLO reaches that goal of 1. Whereas lateral suture (ECR) and TTA fails to reach this goal <10 months post operatively. This means that dogs with a TPLO are much more likely to reach maximum function vs those that have TTA or lateral suture repairs.
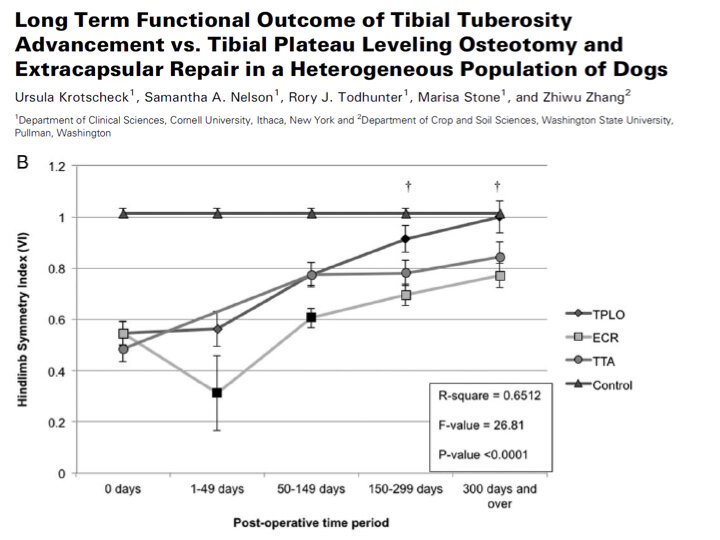
(Vet Surg. 2016 Feb;45(2):261-8. doi: 10.1111/vsu.12445.Epub 2016 Jan 15; Long Term Functional Outcome of Tibial Tuberosity Advancement vs. Tibial Plateau Leveling Osteotomy and Extracapsular Repair in a Heterogeneous Population of Dogs)
A recent systematic review (a summary of published evidence) comparing TTA and TPLO concluded The assessed literature supports the hypothesis that TPLO is associated with lower complication rates, an improved clinical-functional outcome and less increase of OA compared to TTA. The results are indicative for a long-term restoration of normal limb function after TPLO. https://pubmed.ncbi.nlm.nih.gov/30149404/
Ligament substitute
A prosthetic ligament has now been available for many years (lateral extracapsular suture or fabello-tibial suture). Nylon is often used as the substitute ligament, secured by knotting or with a metallic crimp. However, the suture stretches or breaks over time and the patient can return to the pre-operative status in the early phases of recovery. Recently, more robust materials have been developed (Fiberwire®) which do not fatigue in the same way. These techniques may have a better outcome where the injury relates to trauma, as the knee was a ‘normal’ joint prior to injury. With genuine traumatic cranial cruciate ligament ruptures other ligaments may be affected and can be managed using the same ligament substitute material. This is known as a multi-ligamentous or a global knee injury.
I have heard that little dogs don’t need surgery?
This is a frequently uttered statement with very little information to support it. The evidence supporting this statement dates back to the 1970’s and 80’s, when the techniques and expectations of owners and veterinarians alike were very different. Little dogs are not ‘better of’ without surgery. We are strong proponents of early surgical management using techniques that get optimal outcomes. TPLO is recommended for small dogs of all weight ranges at QVS.
Some surgeons claim that it is not possible to perform a TPLO on small dogs, or that is is inherently risky. This is fundamentally incorrect. We regularly perform TPLO on dogs 3kgs and up with excellent success and very low complication rates. They rapidly return to normal activity.
How arduous is the post operative recovery?
Because TPLO is a very safe, predictable, and mechanically robust surgery, the recovery is very manageable but there are precautions that we advise.
Cage or small room confinement for 6 weeks
Regular leash controlled walks, beginning on day 1
Up to 30mins of daily walking is permissible by the end of the 4th week
No off leash running or play for the first 6 weeks
A copy of the typical discharge guidelines post operatively is at the bottom of this page.
How much does surgery cost?
We currently offer a fixed cost of $6000 for patients under 50kg and $6500 for patients weighing over 50kg. This cost is for a single, uncomplicated tibial plateau levelling osteotomy (TPLO). This excludes the cost of the initial consultation.
This includes:
all pre- and immediate post-operative radiographs (x-rays)
all related surgery fees, medication, implant fees
specialist or residency trained surgeon
overnight hospitalisation with 24 hour vet and nurse care
follow up visits (excluding radiographs)
But I found another hospital doing cruciate surgery for much cheaper, why are the costs different?
The cost of providing veterinary care is highly variable. We are committed to keeping surgery costs as low as possible whilst ensuring we can perform the procedure safely at high standards. Cruciate surgery at QVS includes:
Exploration of the joint to inspect the ligament, and meniscus, as well as treat the meniscus (Arthrotomy or arthroscopy)
Local anaesthesia (electrically guided nerve blocks) as well as general anaesthesia
Use of disposable, adhesive, impermeable, 4-quarter drapes as well as a patient/table drape
Use of iodine impregnated, disposable, adhesive limb covers
2 veterinary surgeons operating on each case
Suction, electrosurgery and dedicated theatre lights
Overnight hospitalisation to ensure safe recovery from anaesthesia and
What is the availability of surgery at QVS?
We recognise that seeing your loved one in pain is distressing. We also know that the longer a dog walks around with a ruptured ligament, the greater the risk of secondary meniscal injury (additional pain and worsening arthritis). Having multiple specialists working across multiple hospitals allows us to offer surgery within days of contacting the hospital.
We do ask that you seek a referral from your regular veterinarian before making an appointment.
My dog has not done well after surgery, is there anything that can be done?
Poor outcomes post TPLO are infrequent. But are frustratingly common after some other techniques. Common reasons for poor recovery include:
unresolved, or acquired meniscal injury
infection
ongoing instability
Whilst arthritis is inevitable once the cruciate ligament tears, poor outcomes are not to be expected. Whilst many factors can influence the recovery post surgery, most causes of poor recovery can be resolved. Contact the hospital if you have any concerns regarding your pets recovery. Our surgeons have extensive experience with managing poor outcomes post other procedures and can often offer a solution.