
Medial Patella Luxation
The patella, or kneecap, is a bone that sits in the tendon of the quadriceps muscle. This muscle group is responsible for extending the stifle (knee joint), and for this to occur appropriately, the tendon must remain at the front of the femur. This is achieved by the patella tracking up and down in a groove at the front of the femur (the trochlea), helping to direct the tendon and its associated action across the stifle joint.
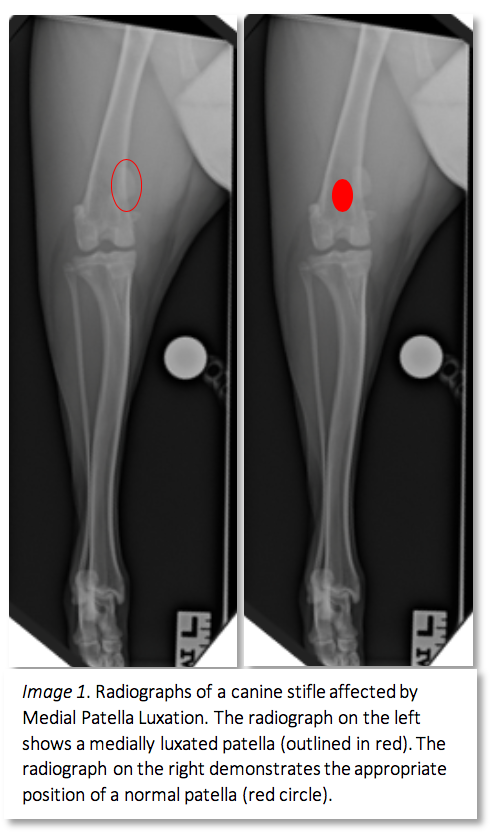
In dogs with Medial Patella Luxation (MPL), the patella slips outside the trochlea, disrupting the mechanism of stifle extension, and can result in secondary changes including angular deformities, cranial cruciate ligament disease and osteoarthritis. These secondary changes result in pain and lameness, and in some cases can become severely debilitating.
Causes of Medial Patella Luxation
There are multiple factors that can lead to a dog developing MPL. It is a condition commonly affecting smaller breed dogs, however larger breeds can still be affected. In smaller breeds, the condition is considered a developmental disease, resulting from congenital deformities affecting the femur (thigh bone), and tibia (shin bone). These changes include coxa vara, femoral varus, and genu varum, which are angular deformities that when combined, give the bow-legged appearance commonly seen in small breed dogs. Dogs with any combination of these hindlimb deformities often also have internal rotation of the tibia and shallow trochlea grooves, which all contribute to the patella’s tendency to luxate medially. While most cases of MPL are considered developmental, occasionally we can see traumatic patella luxations.
Diagnosis
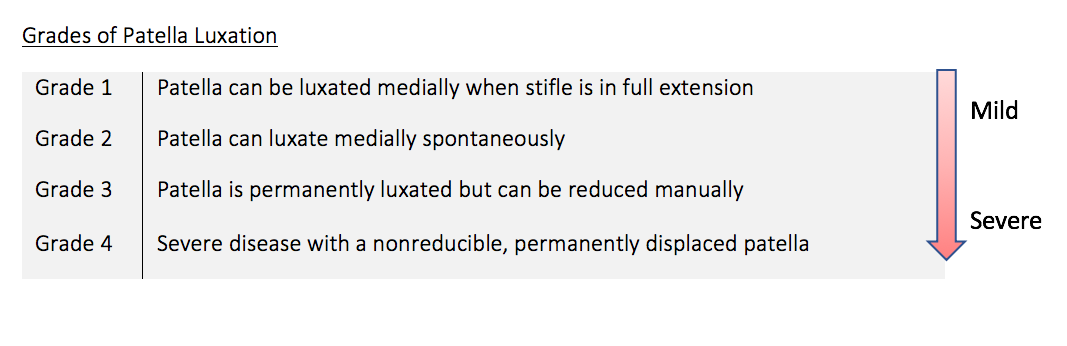
A diagnosis of Medial Patella Luxation is often made based on your pet’s history, and a physical examination. There are varying grades of MPL, with clinical signs varying from mild lameness and intermittent ‘hopping’ or ‘skipping’ on the affected limb whilst running, through to severe lameness and the inability to extend their stifle. In consultation with our surgeons, a full physical examination will be performed, including a thorough musculoskeletal examination. On palpation of your dog’s stifle, the patella will be palpated and determined if there is any luxation that occurs throughout varying degrees of stifle flexion.
Often, there are secondary changes associated with the joint resulting from the MPL, which may include osteoarthritis or concurrent cranial cruciate ligament insufficiency. It is important to identify any other pathology in the joint prior to surgery, as it may alter the approach to treatment. Surgery is best performed early in the disease process, however there are usually options available for even chronically affected dogs.
Surgical Correction
There are several surgical techniques that can be performed to correct a MPL, with a large degree of intraoperative decision making. Some dogs require less correction, whilst other dogs may require all the below procedures to ensure their patella remains in the trochlea.
Trochleoplasty

Many dogs with MPL have a shallow trochlea groove, which can often be associated with poorly developed (or eroded) trochlear ridges. In these cases we will perform a Trochlear Wedge Recession, or a Trochlear Block Recession. These procedures aim to deepen the trochlear groove whilst maintaining the smooth cartilage on which the patella sits. During surgery, a wedge or block of the cartilage surface of the trochlear will be removed temporarily to allow removal of the underlying bone. After sufficient bone has been removed, the trochlea is replaced, now sitting deeper between the trochlea ridges, providing a more appropriate groove for the patella.
Tibial Tuberosity Transposition

There are often angular changes seen in the tibia. These changes result in a medially rotated tibial tuberosity, due to the altered forces of the flexor muscles resulting from the medial luxation. These dogs will have their tibial tuberosity cut and moved laterally to redirect the quadriceps muscle action.
Lateral Imbrication and Medial Release
We often see intra-operatively that the soft tissues surrounding the patella have changed in response to the MPL, notably contracture, or tightening, of the soft tissues and muscles on the medial aspect of the stifle. These changes can continue to pull the patella medially if not corrected, therefore we will often perform a ‘medial release’. This involves creating in incision in the soft tissues that have become contracted to ‘release’ the patella to a normal, central position. Similarly, the lateral tissues can become slack, and can be corrected by performing an overlapping suture (called imbrication) to help maintain the patella in its central position.
Some dogs will have concurrent MPL and Cranial Cruciate Ligament Insufficiency. In these cases, the procedures listed above can be combined with a TPLO to correct both conditions simultaneously. Please refer to the page on Cranial Cruciate Ligament Rupture for further information on these procedures.
Post-operative Management
After MPL corrective surgery, your dog will remain in hospital for 24-48 hours to ensure we have any post-operative pain well controlled prior to discharge. Patients receive multimodal pain relief during their post-operative period, including non-steroidal anti-inflammatories and opioid analgesics.
Once discharged, it is important to ensure your dog remains quiet and confined during their recovery period. In cases where we have performed an osteotomy (trochleoplasty, tibial tuberosity transposition or a concurrent TPLO), your pet will need to remain confined for 6-8 weeks to allow the bone to heal. Confinement is equally important, however, for healing of the soft tissues, especially if lateral imbrication has been performed. During this time, we encourage short (5min) walks on a leash, however boisterous activity and play with other pets should be avoided.